

BACKGROUND:
High-grade B-cell lymphomas (HGBLs) with rearrangement of MYC and BCL2 and/or BCL6, known as "double-hit" or "triple-hit" B-cell lymphomas (DHL/THL), are an aggressive sub-type of non-Hodgkin mature B-cell lymphoma with chromosomal rearrangements involving MYC with BCL2 and/or BCL6 genes. DHL/THLs typically have poor outcomes and early relapses with first-line R-CHOP, and intensive induction chemoimmunotherapy regimens are associated with improved outcomes. Infusional dose-adjusted (DA)-R-EPOCH is commonly used, yet there is a lack of clear evidence that dose-adjustment enhances survival, and variations in compliance with dose-adjustment exist. DA-R-EPOCH has been incorporated as the backbone of prospective clinical trials testing the addition of novel agents for frontline management of DHL/THL, and these combinations may lead to a greater degree of myelosuppression that may disrupt dose-adjustments and hinder dose-escalations relative to using DA-R-EPOCH alone. Therefore, we sought to determine if patients with DHL/THL treated with induction DA-R-EPOCH have differences in clinical outcomes (OS, PFS, treatment-related adverse events and others) based upon compliance with dose-adjustment and cumulative doses of R-EPOCH administered.
METHODS:
Adult (age ≥18 years) patients with DHL/THL treated with induction DA-R-EPOCH chemoimmunotherapy from 2014 to 2019 at six collaborating medical centers were included in this study. To be included, patients must be without CNS-involvement at diagnosis, have received ≥4 cycles of DA-R-EPOCH, have adequate clinicopathologic data regarding chemoimmunotherapy dosing, survival, treatment response/remission status, cell counts, CNS and antimicrobial prophylaxis, admissions for cytopenias or IV antibiotics, and demographic data including age, international prognostic index (IPI), CNS-IPI, ECOG performance status, and cumulative illness rating score (CIRS, if available). An initial cycle of R-CHOP was permitted. De-identified data from participating sites were combined, and chemotherapy doses were aggregated and divided into quartiles based on cumulative doses of doxorubicin, etoposide, and cyclophosphamide received. Correlation between CIRS and dose was assessed by Spearman's correlation. OS and PFS were estimated using the Kaplan-Meier method and compared using log-rank test.
RESULTS:
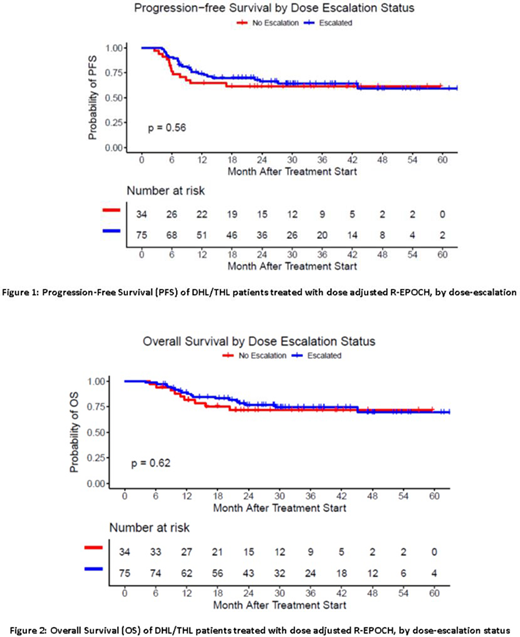
109 total patients were included in this study. The median age was 63 years (range 29-83), and approximately 60% of patients were male, 58% were age 60 or older, 60% had an IPI score of ≥3, and 66% were Ann Arbor Stage IV at induction. For all patients, 2-year and 5-year OS rates were 75% (95% CI: 67-84%) and 70% (59-82%), with 27 total deaths in the study period. 2-year and 5-year PFS rates were 65% (56-75%) and 60% (49-72%), respectively. 94 of 109 patients received CNS prophylaxis (86%). 26 patients had received an initial cycle of R-CHOP (24%). PFS and OS were significantly worse for patients with higher risk IPI score (P = 0.03, 0.04, respectively), but there was no difference in PFS or OS based on CIRS score (P = 0.70, 0.60, respectively). 75 patients (68.8%) were dose-escalated while 34 patients (31.2%) were not; there was no difference in PFS (Fig 1) or OS (Fig 2) between these groups. When stratified by cumulative dose-level in quartiles, those who received the lowest cumulative doses (1st quartile) had a significantly reduced OS (1st, 2nd, 3rd and 4th quartile 2-year OS of 55%, 75%, 85%, and 84%, P = 0.046). Cause of death was largely from disease progression (74%), with only one treatment-related death in each dosing quartile. Dose intensity was not correlated with baseline CIRS score (R = -0.06, P = 0.56), but did correlate negatively with IPI (R = 0.22, P = 0.04).
CONCLUSIONS:
OS and PFS did not differ for DHL/THL patients treated with R-EPOCH with dose-escalation in at least one cycle as compared to those with no dose-escalation. Although cumulative doses beyond the 1st quartile were associated with improved OS, there was no significant difference between 2nd, 3rd and 4th quartiles. Dose-escalation was negatively associated with IPI scores but not CIRS scores. Further investigation into factors affecting adherence to dose-adjustment is warranted. The effect of adding novel agents to the DA-R-EPOCH backbone on dose-adjustment and cumulative doses of chemotherapeutic agents received should be evaluated in prospective clinical trials.
Haverkos:Viracta THerapeutics: Consultancy. Hughes:Acerta Pharma and HOPA: Research Funding; AstraZeneca: Consultancy; Genzyme: Consultancy; Janssen: Consultancy; AbbVie: Consultancy. Grover:Genentech: Research Funding; Tessa: Consultancy. Portell:Amgen: Consultancy; Bayer: Consultancy; BeiGene: Consultancy, Research Funding; Kite: Consultancy, Research Funding; Acerta/AstraZeneca: Research Funding; Xencor: Research Funding; Roche/Genentech: Consultancy, Research Funding; Infinity: Research Funding; TG Therapeutics: Research Funding; AbbVie: Research Funding; Pharmacyclics: Consultancy; Janssen: Consultancy. Voorhees:AstraZeneca: Research Funding. Landsburg:Triphase: Research Funding; Seattle Genetics: Speakers Bureau; Celgene: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Curis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Morphosys: Membership on an entity's Board of Directors or advisory committees; Takeda: Research Funding. Kahl:Genentech: Consultancy; Pharmacyclics LLC: Consultancy; BeiGene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca Pharmaceuticals LP: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene Corporation: Consultancy; AbbVie: Consultancy; Roche Laboratories Inc: Consultancy; Acerta: Consultancy, Research Funding; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees; ADC Therapeutics: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding. Hill:Takeda: Research Funding; Karyopharm: Consultancy, Honoraria, Research Funding; Pharmacyclics: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria, Research Funding; AstraZenica: Consultancy, Honoraria, Research Funding; Kite, a Gilead Company: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria; Genentech: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; Beigene: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal